Why Economic Growth Is Good for Your Health

Viewpoint examining the robust positive relation between economic growth in freer societies and our ability to lead longer, healthier lives
There is a connection between economic growth and increased life expectancy, concludes this study published by the MEI. “With some people calling for ‘degrowth,’ it’s worth remembering that a wealthier world is a healthier world,” says Vincent Geloso, Senior Economist at the MEI and author of the study.
 Related Content
Related Content
 |
 |
 |
| Economic growth is good for your health (Sun Media Papers, April 27, 2023)
Live long and prosper! They go together (Western Standard, April 30, 2023) |
Interview (in French) with Vincent Geloso (Mario Dumont, QUB Radio, April 27, 2023) |
This Viewpoint was prepared by Vincent Geloso, Assistant Professor of Economics at George Mason University and Senior Economist at the MEI. The MEI’s Health Policy Series aims to examine the extent to which freedom of choice and entrepreneurship lead to improvements in the quality and efficiency of health care services for all patients.
It is popular in certain circles to attack the very idea of economic growth. One criticism sometimes made is that countries like the United States that are exceptionally rich by global standards have lower levels of life expectancy at birth than countries of more modest wealth. Yet the positive relation between economic growth and life expectancy is far more robust than suggested by such simple comparisons. In fact, the institutions that generate economic growth are both directly and indirectly tied to our ability to lead longer—and healthier—lives.
The idea of a connection between economic growth and health outcomes has a long tradition.(1) The generally advanced mechanism is that higher incomes are associated with better and more stable diets that ward off multiple diseases and avoid stunting during periods of privation.(2) This effect is particularly strong for children who reap clear nutritional benefits in their formative years thanks to their parents’ higher incomes. In turn, these improved health outcomes also stimulate economic growth, as people who live longer, healthier lives tend to be more productive, creating a virtuous cycle.(3)
This direct channel, however, does not explain the majority of declines in mortality (and thus improvements in life expectancy).(4) While it is quite strong at low levels of income and life expectancy, so that initial increases in income can have large positive effects, these improvements shrink beyond a certain income level. Thus, while more income is always beneficial to health outcomes, it is decreasingly so as a country grows richer.(5)
Many thus emphasize the role of public health interventions as the driver of improvements at higher income levels.(6) There are, however, three problems with disregarding the important role of economic growth in improving health and longevity. First, there is a large share of the global population that remains quite poor and thus stands to benefit mightily from economic growth. Second, government interventions tend to be more effective in richer societies, as economic growth enables interventions or permits the development and deployment of new technologies by the public sector.(7) Third, and most importantly, there is a biological frontier to life expectancy explaining the declining health returns from economic growth.
A Better Life Expectancy Metric
Substantial life expectancy improvements are easier to achieve from a low level than from a high level. This increasing difficulty for purely biological reasons makes it nearly automatic that improvements from economic growth would taper off. These biological limits are difficult (but not impossible) to push.
Moreover, countries that are nearer to these limits have enjoyed considerable declines in the proportion of life spent in disability, with older people more likely to still be physically and mentally healthy.(8) Given that the quality of each year lived matters, not just the number of years lived, using simple life expectancy at birth as a metric can miss an important part of the picture.
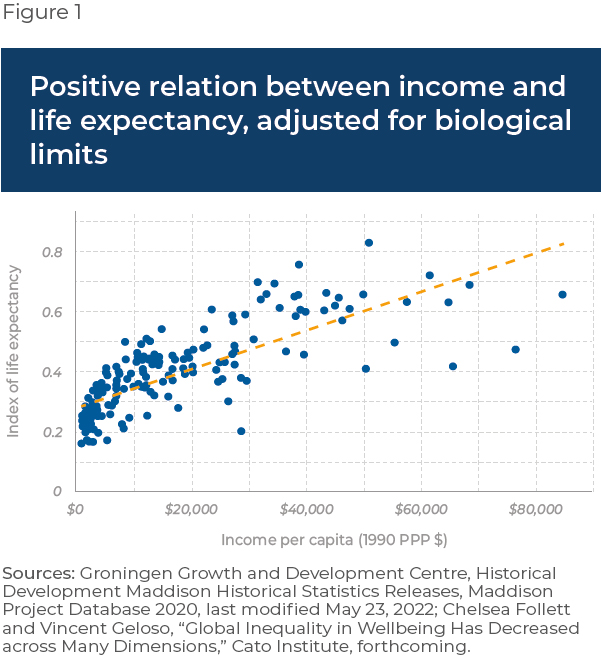
This is why many economists suggest using an index of life expectancy that gives more weight to achievements near our biological limits.(9) After all, it is far more impressive to increase life expectancy by a year when many live to 85 and beyond than when the average lifespan is just 35. Figure 1 depicts the adjusted correlation generally employed by these economists.(10) As can be seen, there are no diminishing effects of income on our ability to secure equally difficult improvements in health outcomes.
The Role of Drug Innovation & Institutions
A potent illustration of our ability to tackle difficult health issues once we become wealthier can be seen in the role of pharmaceutical drug development. Constant biopharmaceutical innovation has allowed for the treatment of diseases once considered incurable. This has not only reduced mortality rates, but it has also reduced disability rates so that healthy life expectancy has increased.
One study of 52 countries found that the development of new drugs explained 40% of the gains in life expectancy from 1986 to 2000.(11) Other studies have shown that a sizable share of these gains in rich countries like the United States and New Zealand come from reductions in mortality risks after age 65.(12)
The investments necessary to develop new drugs are far easier to make in rich societies that can afford to spend more on research and development.(13) Moreover, the researchers, innovators, and entrepreneurs who undertake long, expensive drug research and development projects need a guarantee that the fruits of their labour will not be confiscated or diminished by government fiat.
This is why elements of economic freedom—notably the protection of property rights and unhampered market prices—are intimately tied to the ability to make such investments. Economically free societies also generally enjoy far faster rates of economic growth and higher levels of income than less free societies,(14) which again directly foster the development of new medical care techniques and biopharmaceuticals.(15)
Simply put, one cannot disentangle the institutions that generate economic growth from those that generate improved health outcomes for the population.
References
- Thomas McKeown, The Modern Rise of Population, Edward Arnold, 1976; M. C. Buer, Health, Wealth and Population in the Early Days of the Industrial Revolution, London Routledge and Kegan Paul, 1926.
- Bernard Harris, “Public Health, Nutrition, and the Decline of Mortality: The McKeown Thesis Revisited,” Social History of Medicine, Vol. 17, No. 3, December 2004, pp. 379-407.
- Lorenzo Rocco et al., “Mortality, morbidity and economic growth,” Plos one, Vol. 16, No. 5, May 2021, p. 9.
- Jonathan Chapman, “The contribution of infrastructure investment to Britain’s urban mortality decline, 1861-1900,” The Economic History Review, Vol. 72, No. 1, February 2019, pp. 233-259.
- Samuel H. Preston, “The changing relation between mortality and level of economic development,” Population Studies, Vol. 29, No. 2, July 1975, pp. 231-248.
- Louis Cain and Elyce Rotella, “Death and spending: Urban mortality and municipal expenditure on sanitation,” Annales de démographie historique, Vol. 101, No. 1, 2001, p. 143.
- Werner Troesken, The Pox of Liberty, University of Chicago Press, 2015; Werner Troesken, “Typhoid Rates and the Public Acquisition of Private Waterworks, 1880-1920,” Journal of Economic History, Vol. 59, No. 4, December 1999, pp. 927-948; Vincent Geloso, Kelly Hyde, and Ilia Murtazashvili, “Pandemics, economic freedom, and institutional trade-offs,” European Journal of Law and Economics, Vol. 54, No. 1, 2022, pp. 37-61.
- Simon I. Hay et al., “Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016,” The Lancet, Vol. 390, September 16, 2017, p. 1260.
- Leandro Prados de la Escosura, “Health, Income, and the Preston Curve: A Long View,” Economics and Human Biology, Vol. 48, January 2023, pp. 8-9; Nanak Kakwani, “Performance in living standards: An international comparison,” Journal of Development Economics, Vol. 41, No. 2, 1993, pp. 307-336.
- This is known as a Kakwani transformation and takes this mathematical form:

- Frank Lichtenberg, “The Impact of New Drug Launches on Longevity: Evidence from Longitudinal Disease-Level Data from 52 Countries, 1982-2001,” NBER Working Paper, (w9754), June 2003, p. 1.
- Frank Lichtenberg, “The Impact of New Drugs on US Longevity and Medical Expenditure, 1990–2003: Evidence from Longitudinal, Disease-Level Data,” The American Economic Review, Vol. 97, No. 2, May 2007, pp. 438-443; Frank Lichtenberg, “The impact of pharmaceutical innovation on the longevity and hospitalization of New Zealand cancer patients, 1998–2017,” Expert Review of Pharmacoeconomics & Outcomes Research, Vol. 21, No. 3, March 15, 2021, pp. 457-475.
- Paul Heney, “Global R&D investments unabated in spending growth,” R&D World, March 19, 2020.
- Joshua Hall and Robert Lawson, “Economic Freedom of the World: An Accounting of the Literature,” Contemporary Economic Policy, Vol. 32, No. 1, January 2014, pp. 1-19.
- Yi Qian, “Do National Patent Laws Stimulate Domestic Innovation in a Global Patenting Environment? A Cross-Country Analysis of Pharmaceutical Patent Protection, 1978–2002,” The Review of Economics and Statistics, Vol. 89, No. 3, August 2007, p. 436.